
The Science and History of Psychedelics: How They Work and Where the Research Stands in 2026
For most of the last century, psychedelics lived in the cultural margins, bound up with the counterculture of the 1960s, criminalized, and effectively walled off from serious study. That era is ending. A wave of rigorous neuroscience, late-stage clinical trials, and shifting federal policy has moved these compounds from the fringe toward the center of psychiatry. This guide explains what psychedelics are, how they act on the brain, the experiences they produce, the history that shaped their reputation, and exactly where the science and regulation stand in 2026.
What are psychedelics?
Psychedelics are a class of psychoactive compounds that temporarily alter perception, mood, cognition, and the sense of self by acting primarily on serotonin receptors in the brain. The word was coined in 1957 by British psychiatrist Humphry Osmond, who combined the Greek psyche ("mind" or "soul") and deloun ("to manifest") to mean "mind-manifesting."
The terminology itself carries a hidden history of bias. In the late 1960s, many researchers preferred psychotomimetic, literally "psychosis-mimicking", on the assumption that these drugs modeled mental illness. When that framing proved inaccurate, the field shifted to hallucinogen, which is still standard in scientific writing despite being imprecise: at typical doses, most people do not experience true hallucinations. The modern preference is to reserve the term classic serotonergic psychedelics for compounds that act as agonists at the brain's serotonin 5-HT2A receptor.
How do psychedelics work in the brain?
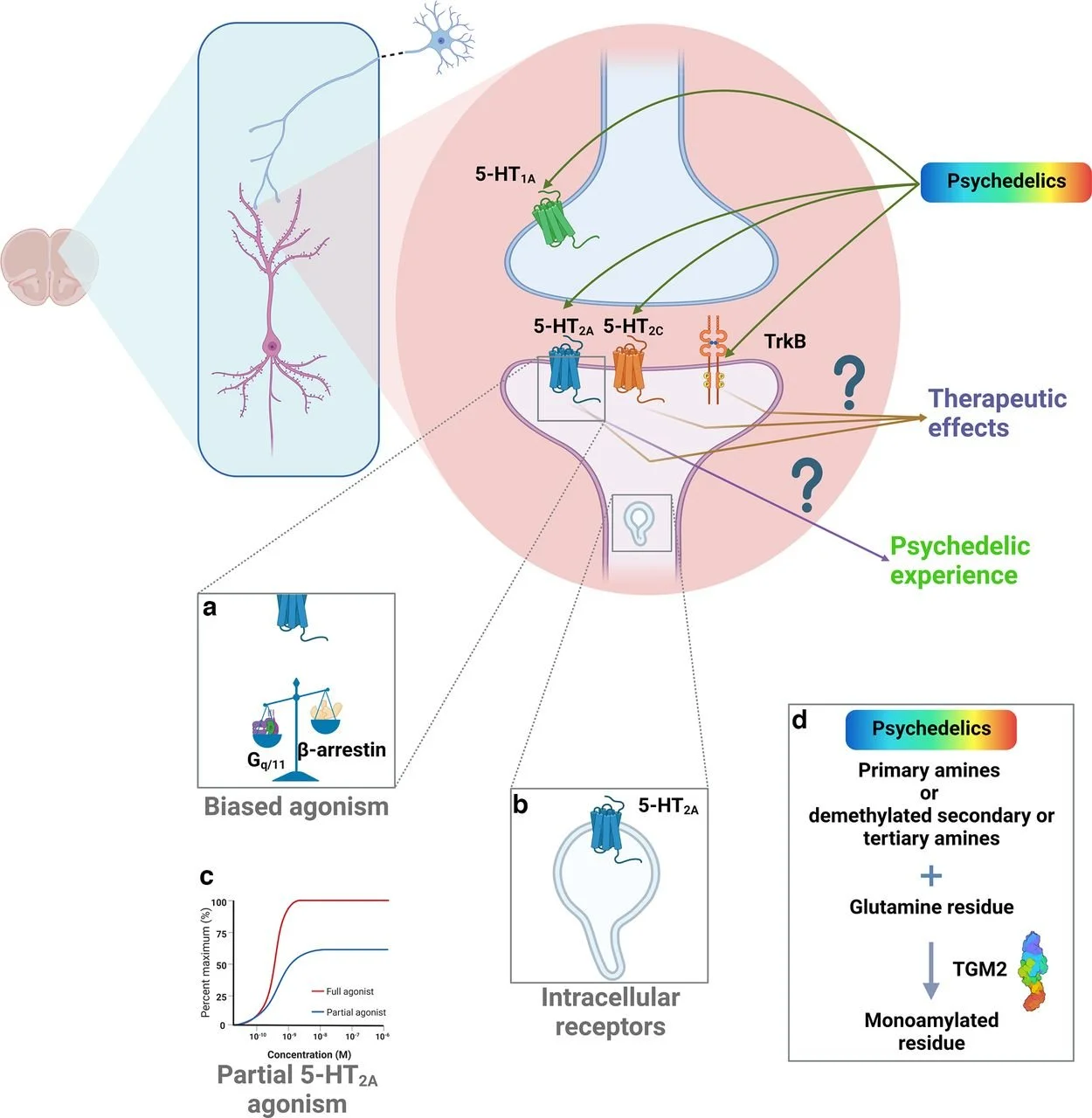
Classic psychedelics work by binding to and activating the serotonin 5-HT2A receptor, which reshapes activity across the brain networks responsible for perception, cognition, and self-referential thought.
The 5-HT2A receptor is a G protein-coupled receptor found throughout the central nervous system. It helps modulate the release of several neurotransmitters, including dopamine, norepinephrine, and acetylcholine, and influences mood, anxiety, appetite, learning, and memory. When a psychedelic binds to this receptor, it changes the firing patterns of key cortical and subcortical circuits, particularly those that integrate sensory information and sustain our ordinary sense of being a continuous "self."
Two downstream consequences matter most for therapy. The first is altered network connectivity, psychedelics loosen the brain's habitual wiring and let normally separate regions communicate. The second is neuroplasticity, animal studies show psychedelics promote the growth of new synaptic connections in the cortex and hippocampus, the cellular machinery of learning and lasting change.
What are the main classic psychedelics?
Most classic psychedelics belong to one of three chemical families: tryptamines, phenethylamines, or lysergamides. Four compounds account for the bulk of both research and traditional use.
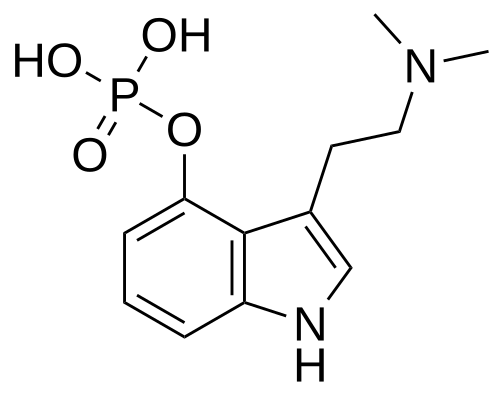
Psilocybin
Compound: Psilocybin
Chemical family: Tryptamine
First characterized: Isolated by Albert Hofmann, 1957–58
Natural source: Found in over 100 mushroom species (e.g., Psilocybe spp.)
Hallmark effects: Altered perception of time and space; shifts in mood and meaning; the most clinically advanced psychedelic
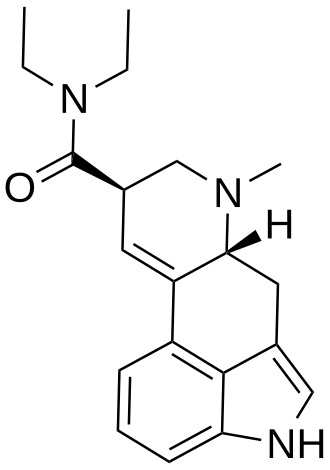
LSD
Compound: LSD
Chemical family: Lysergamide
First characterized: Synthesized by Albert Hofmann, 1938; psychoactivity found 1943
Natural source: Derived from ergot, a fungus that grows on rye
Hallmark effects: Intensified thought, emotion, and sensory perception; long duration
Mescaline
Compound: Mescaline
Chemical family: Phenethylamine
First characterized: Isolated 1897; synthesized 1919
Natural source: Peyote, San Pedro, and Peruvian torch cacti
Hallmark effects: Altered self-awareness and time sense; geometric visual patterning
DMT
Compound: DMT
Chemical family: Tryptamine
First characterized: Synthesized 1931; effects characterized by Stephen Szára in the 1950s
Natural source: Many plants; the active component of the brew ayahuasca
Hallmark effects: Rapid, intense, immersive states with profound perceptual distortion
Each produces a distinct profile, but all share the same core mechanism: 5-HT2A agonism.
What is the psychedelic experience actually like?
There is no single "psychedelic experience." The effects depend on the specific compound, the dose, and, critically, the person's mindset and surroundings, a pairing researchers call set and setting.
In general, lower doses produce sensory shifts: heightened color, repeating geometric patterns, and changes in how time feels. Higher doses can produce far more profound alterations, including the temporary dissolution of the boundary between self and world, an effect often described as ego dissolution. These states are frequently, though not always, accompanied by positive mood and a sense of personal meaning. They are also unpredictable, which is precisely why screening, preparation, and supervision matter.
To make sense of this variability, psychiatrists Robin Carhart-Harris and David Nutt proposed an extra-pharmacological model of drug action in 2017. It holds that the outcome of a psychedelic experience is shaped not only by the drug and dose but by a wider set of factors:
Trait factors — biology, personality, and suggestibility
Pre-state — expectations, anticipatory anxiety, and willingness to "let go"
State — the acute subjective and biological quality of the experience
Setting — the physical and social environment
Long-term outcomes — lasting effects on symptoms, outlook, and personality
The practical lesson is that the molecule is only part of the story. Underestimating the non-drug factors can make these experiences riskier, which is why responsible clinical and supervised models invest so heavily in preparation and integration.
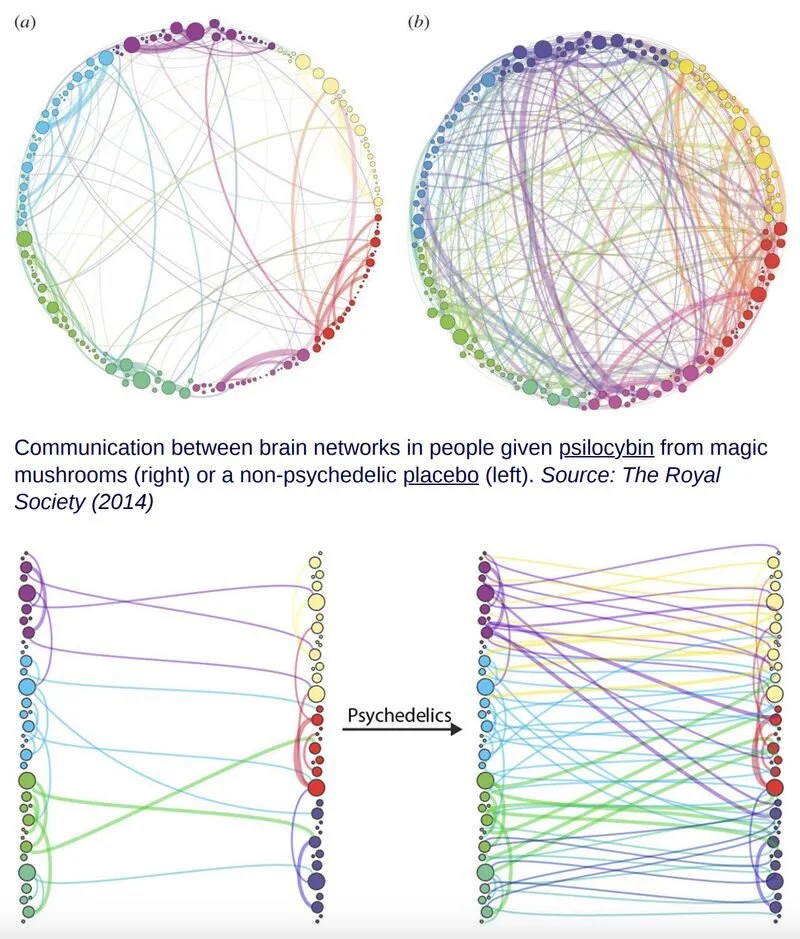
What does brain imaging reveal about the psychedelic state?
Modern neuroimaging shows that psychedelics temporarily reorganize how the brain's large-scale networks communicate, quieting the system tied to habitual self-focus while increasing cross-talk between regions that are normally segregated.
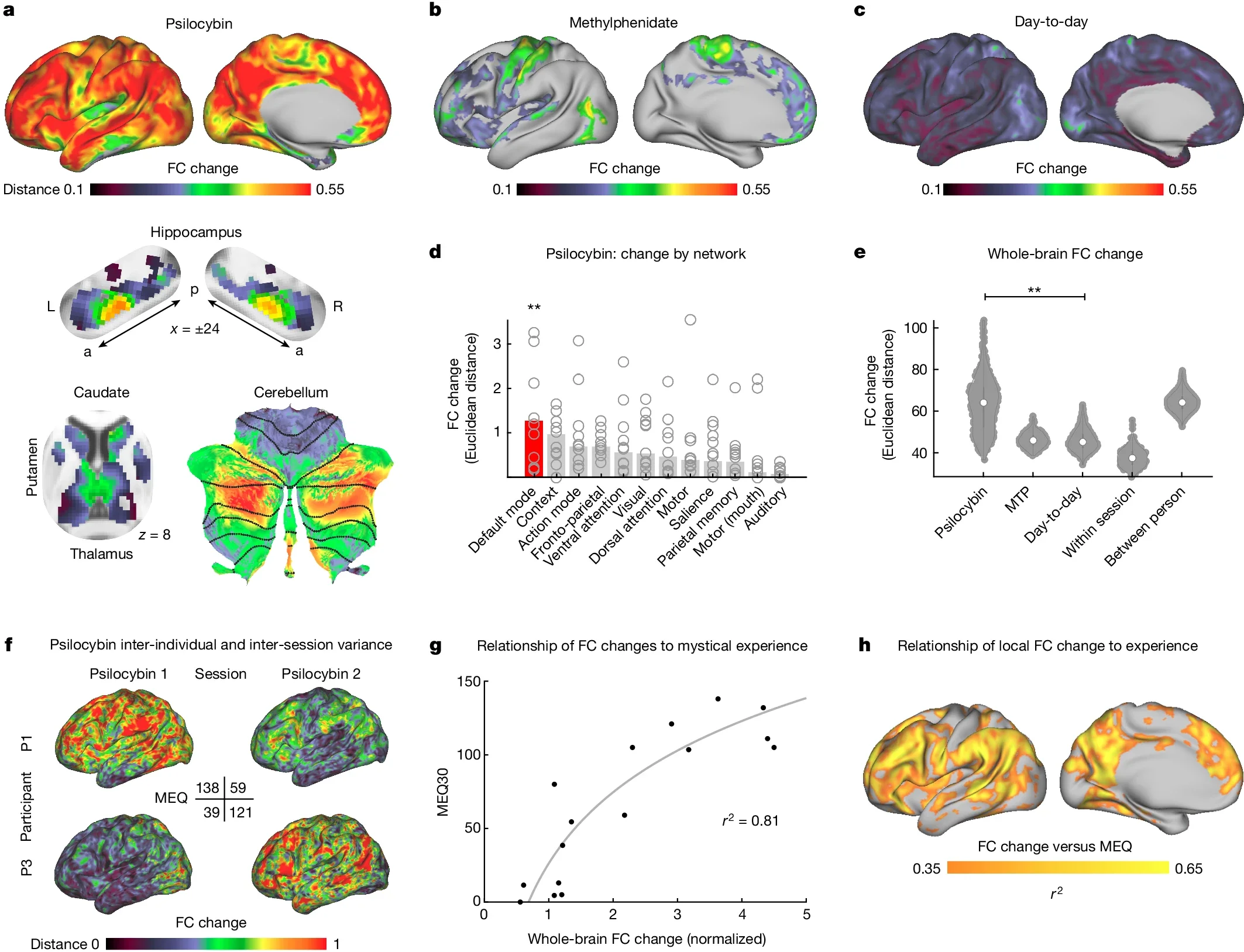
Much of this work has centered on the default mode network (DMN), a set of regions associated with mind-wandering, self-reflection, rumination, and autobiographical memory. Early studies found that psilocybin reduces DMN activity and connectivity while allowing distant brain regions to form new, temporary functional links, a pattern researchers connect to the dissolution of rigid self-identity.
The most rigorous evidence to date arrived in a 2024 study published in Nature. Using precision functional mapping, roughly 18 brain scans per participant before, during, and for weeks after dosing, researchers found that a single 25 mg dose of psilocybin massively disrupted functional connectivity across the cortex and subcortex, producing more than three times the change seen with a stimulant comparison drug. Crucially, some of these network changes persisted after the acute experience faded, offering a plausible neural signature for why a single session can produce lasting psychological effects. This desynchronization, paired with the renewed plasticity seen in animal models, may explain the durability that distinguishes psychedelics from many conventional treatments.
A brief history of psychedelics
Psychedelic plants and fungi have been used in ritual and healing contexts for thousands of years, long predating modern chemistry. Archaeological and ethnographic evidence points to ceremonial use across the Americas dating back millennia, where communities cultivated deep, structured relationships with these substances.
Western science engaged them seriously only in the twentieth century. Hofmann's accidental discovery of LSD's effects in 1943 launched two decades of legitimate psychiatric research, with thousands of studies exploring applications for addiction, anxiety, and depression.
That trajectory collapsed in the 1960s. As psychedelics became entangled with anti-war protest and rejection of mainstream norms, a political backlash followed. The Controlled Substances Act of 1970 placed LSD, psilocybin, and other psychedelics in Schedule I, the most restrictive federal category, effectively ending clinical research for more than three decades. The speed of adoption, the absence of cultural guardrails, and widespread misunderstanding all contributed to the shutdown. The science didn't fail; the cultural moment did.
The psychedelic renaissance: where the field stands in 2026
After thirty years of dormancy, psychedelic research has re-emerged with unprecedented momentum, and 2026 has been its most consequential year yet. The renaissance is no longer just academic; it is clinical, regulatory, and federal.
The clinical frontier. Compass Pathways' COMP360, a synthetic, pharmaceutical-grade psilocybin for treatment-resistant depression, is the most advanced classic psychedelic in development. It achieved positive results in two consecutive Phase 3 trials, COMP005 in June 2025 and COMP006 in February 2026, meeting its primary endpoints with high statistical significance and showing durable improvement from a supervised single 25 mg dose. The company is targeting a rolling new drug application submission in Q4 2026. If approved, COMP360 would become the first classic psychedelic ever cleared by the U.S. Food and Drug Administration. The nonprofit Usona Institute is advancing psilocybin for major depressive disorder on a parallel track, building on Phase 2 results published in JAMA in 2023 that showed a rapid and sustained antidepressant effect.
A federal turning point. On April 18, 2026, a presidential executive order directed federal agencies to accelerate research on Schedule I psychedelics, including psilocybin, LSD, MDMA, and ibogaine, through Breakthrough Therapy designations, priority regulatory review, at least $50 million in funding, and explicit partnership with states running their own programs. The order does not, by itself, approve any drug or lower the FDA's evidentiary bar, but it signals a decisive shift in federal posture. Days later, on April 24, the FDA issued National Priority Vouchers to Compass, Usona, and Transcend Therapeutics, a pilot mechanism that can compress the standard 10-to-12-month review down to one or two months.
A cautionary tale. The path is not frictionless. In August 2024, the FDA declined to approve MDMA-assisted therapy for PTSD from Lykos Therapeutics (the drug-development company that grew out of MAPS), issuing a Complete Response Letter and requesting an additional Phase 3 trial. The decision underscored how difficult it is to win approval for a protocol that combines a drug with psychotherapy, and why the furthest-advanced programs now emphasize conventional, rigorously designed drug trials.
State-level access. While federal approval is pending, regulated state programs have quietly built real-world infrastructure. Oregon's supervised psilocybin service centers have served roughly 16,000 clients since launch. Colorado now has dozens of licensed healing centers operating under its Natural Medicine Health Act. And in April 2025, New Mexico became the first state to legalize medical psilocybin through legislation. Psilocybin nonetheless remains a Schedule I substance at the federal level as of mid-2026, a tension between state practice and federal law that defines the current moment.
What conditions might psychedelics treat?
Research suggests psychedelics may help treat several mental health conditions that respond poorly to existing medications, most notably depression, PTSD, anxiety, and substance use disorders.
The strongest evidence is in depression, where supervised psilocybin sessions have produced rapid and sustained reductions in symptoms in controlled trials. Other lines of research point to reduced anxiety in people facing life-threatening illness, and to improvements in alcohol, tobacco, and other substance use disorders. An emerging and less expected finding is that psychedelics may also have anti-inflammatory properties: in animal models, classic psychedelics suppressed inflammatory markers in conditions such as asthma, hinting at therapeutic potential well beyond psychiatry.
A parallel effort aims to separate the therapeutic benefits from the trip itself. Researchers are designing non-hallucinogenic psychedelic analogs that activate the beneficial 5-HT2A pathways and promote plasticity without producing the intense subjective experience — which could make treatment easier to scale and supervise. Whether the subjective experience is essential to the healing, or incidental to it, remains one of the field's central open questions.
Why trained, supervised settings matter
The single most consistent lesson from both the research and the regulatory record is that outcomes depend on context, not just chemistry. The same dose can produce healing or harm depending on screening, preparation, the environment, and the skill of the person holding the space.
That is why the renaissance has produced a parallel need: qualified professionals trained to guide these experiences safely and ethically. Rigorous screening protocols help identify who is, and isn't, a good candidate; structured preparation and integration shape whether an experience becomes durable benefit; and trauma-informed, ethically grounded practice protects people at their most vulnerable. As legal access expands across Oregon, Colorado, New Mexico, and the states preparing to follow, the field's bottleneck is increasingly human, not pharmacological.
Changa Institute is the nation's first government-accredited psilocybin facilitator training program, preparing practitioners across Oregon, Colorado, and New Mexico to meet exactly this need, pairing scientific rigor with the care these medicines demand.
Frequently asked questions
What is a psychedelic? A psychedelic is a psychoactive compound that temporarily alters perception, mood, and the sense of self by acting on the brain's serotonin 5-HT2A receptors. The main classic psychedelics are psilocybin, LSD, mescaline, and DMT.
How do psychedelics work? Classic psychedelics activate the serotonin 5-HT2A receptor, which reorganizes communication across large-scale brain networks and promotes neuroplasticity, the growth of new synaptic connections involved in learning and lasting change.
Are psychedelics legal in the United States? Psilocybin and other classic psychedelics remain Schedule I controlled substances under federal law as of 2026. However, Oregon and Colorado run regulated supervised-use programs, and New Mexico legalized medical psilocybin in 2025.
Is psilocybin FDA approved? Not yet. As of 2026, Compass Pathways' COMP360 psilocybin has completed two positive Phase 3 trials for treatment-resistant depression and is on track for an FDA submission, which could make it the first classic psychedelic approved in the U.S.
What conditions are psychedelics being studied for? Active research focuses on treatment-resistant depression, major depressive disorder, PTSD, end-of-life anxiety, and substance use disorders, with emerging interest in anti-inflammatory applications.
What does "set and setting" mean? Set and setting refers to a person's mindset (set) and their physical and social environment (setting). Both strongly influence the nature and outcome of a psychedelic experience, which is why supervised, prepared contexts matter.